The levels and phases of creative ability

Levels of creative ability
There are nine levels of creative ability, representing the full scope of human beings.
Each level is comprised of volition corresponding with action, therefore each level has a term describing the volition and a term describing the action that is seen as an expression of the volition. See the graphic of the model on the page -THE VdTMoCA IN DETAIL.
The first level of human life is the volitional level of Tone (to survive, exist, with needs therefore for food, comfort, safety similar to the first level of Maslow's Hierarchy of Needs), which corresponds to action termed unplanned (reflexive, instinctive rather than consciously planned). The last level is Competitive Participation (volition),Society-centred (action). The levels are described in a lot of detail by Casteleijn & Holsten (2019).
The levels represent the shift from a focus on the self in the usual course of development (Tone to Self-presentation), to growth into a desire for Participation (Passive-Active Participation), and finally growth into having more volition for benefiting others rather than the self, prepared to sacrifice own needs (Competitive to Competitive Contribution) - few people grow into these levels (e.g. Nelson Mandala, Dali Lama).
De Witt (2005, p.19) grouped the levels according to three discrete stages (Table 1). An explanation of grouping the levels is also provided by Casteleijn & Holsten (2019). 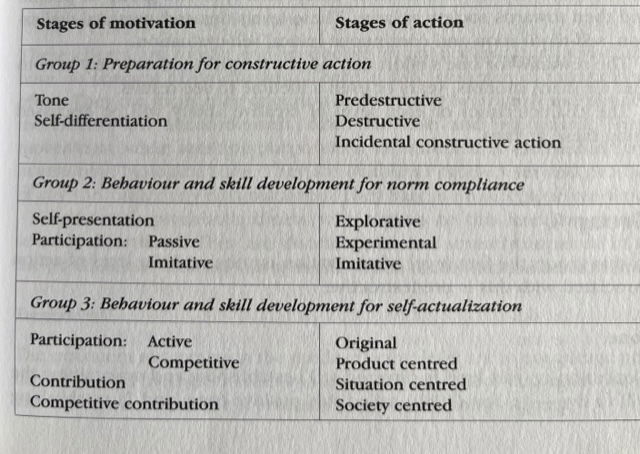
Table 1. The groups into which creative ability can be divided (De Witt, 2005, p.19)
The levels are sequential. There can be upwards growth and downwards decline or regression as a natural course of life. There is a gradual transition from one level into the next, as represented by the gradually changing colour of the levels from one to the next/previous level. Growth is in breadth and depth, represented by the increasing in depth and breadth of the spiral. Decline is a reduction in depth and breadth.
Specific levels of creative ability can be expected to be seen in certain services. The earlier/lower the level, the greater the need for support, supervision. At Tone, 24 hour care is needed. As one progresses through the levels, there is less need for care and greater rehabilitation potential (Venter & Zietsman, 2005) (Fig. 1).

Figure 1. A model of care, treatment and rehabilitation required based on Du Toit's levels of Creative Ability (Venter & Zietsman, 2005, p.200). NB this figure has presented the sequence of the levels differently to the VdTMoCA, placing the level of Tone at the top. You might find it helpful to reproduce this figure the other way around for your CPD.
The usual adult levels are Self-presentation to Active Participation, most adults probably being on Passive Participation and Imitative Participation. Self-presentation is the level predominantly seen in health and social care.
With the growing widening of the scope of OT to work with people in wellness, in business, and displaced by war and climate change, there is greater interest in the Active Participation and later levels, which are less known in healthcare (Grobler, 2009; Joubert, 2021). Subsequently, there has been a call for OTs to research these levels.
Phases of creative ability
Movement through a level occurs in three phases. In progression or growth through a level, order is therapist-directed phase (TDP), patient-directed phase (PDP) and transitional phase (TP). The phases indicate how far into the level a person is - at what stage they are. At the beginning of the level (TDP), one would not expect a person to have as much ability as at the end of the level, moving into the next level (TP). Essentially, this is what the phases capture.
The phases indicate the amount and quality of creative ability that the individual has on any given level. Subsequently, the amount and quality of ability indicates the amount and quality of assistance, facilitation, support or supervision a person therefore needs. Therefore, the phases are extremely helpful for gauging how to work with an individual. This is illustrated by the following key words describing the therapeutic input, explained in detail by Van der Reyden at al, 2019a).
Upgrading demands supports progression through the levels; downgrading should occur in response to signs of regression.
Therapist-directed phase (TDP)
The therapist invites the person to respond and participate. This requires the therapist to facilitate the person’s awareness of him/herself, the activity (materials, objects), people and the surrounding environment.
Every attempt and exertion of effort by the person is nurtured by the therapist, therefore, the therapist needs to be closely present. Activity participation should include repetition, practice and reinforcement.
Patient-directed phase (PDP)
The therapist’s focus changes to that of enhancing, consolidating, stabilising, and/or expanding the person’s knowledge, skills and/or abilities. Activity participation is graded to provide the just right challenge (new experiences), which are repeated to reinforce knowledge and skill are reinforced.
Some therapists have changed the wording of this phase to person-directed phase. Certainly, the term 'patient' does not relate to people who are in wellness or simply not a patient, so the terminology might change in the future, but in the meantime, it is important to use the terminology of the model unless contraindicated. Feel free to contact wendy@ican-uk.com if you want to put forward suggestions for changing any terminology.
Transitional phase (TP)
The therapist’s focus is on further consolidation and expansion of ability and skill, plus challenging the person to greater exertion of effort to move to the next level. Strategies that may be useful when there are emerging characteristics of the next level, are using graded exposure and anticipation (planning, prediction); creating opportunities within a safe environment to explore, experiment or practise. Once the person has gained a degree of competence or mastery, exposure to selected challenges in keeping with the emerging characteristics may be therapeutic.
The transition takes the person into the next level where the challenges are greater therefore the person starts again at the therapist-directed phase (Fig. 2)

Figure 2. Progression through the phases of creative ability from one level of creative ability to the next. Training image by Sherwood (2023)
The movement from one level into the next is captured in the ICAN logo, indicating growth.
Difference between therapist-directed and transitional phase
During the TP, there is a focus on consolidation and reinforcement of the current level, while nurturing the emerging characteristics of the next level. In the TDP, the focus is on facilitating and nurturing the emerging characteristics of the current level, while reinforcing newly acquired abilities.
A distinct benefit of being able to recognise changes in a person's phase of creative ability, is that therapists are closely attuned to the person. When a peson improves or deteriorates slightly, the therapist can change the input accordingly. In this way, the therapist moves alongside the person, responding to changing needs.
Furthermore, small changes as in a change of phase can be measured. It has been openly discussed in practice that many measures used by OTs, especially in mental health are not sensitive enough to capture changes - the therapist has seen the person change, but on rescoring the measure does not indicate any change. In using the VdTMoCA, small changes, which can be extremely significant changes, can be captured. Carter (2013) identified that for adults admitted into an inpatient acute mental health service, a change in the phase of a level most frequently occurred by discharge rather than improvement by a whole level of creative ability. This is important to know and communicate to the clinical team and commissioners.